- Implicit bias refers to automatic, unconscious assumptions that shape clinical judgment without the clinician’s awareness.
- Research consistently shows that mental health providers hold implicit biases at comparable rates to the general population.
- In clinical settings, these biases can influence diagnosis, treatment planning, and the quality of care provided to different client groups.
- Bias cannot be fully eliminated, but it can be actively managed through self-awareness, structured protocols, and ongoing training.
- Addressing implicit bias is an ongoing ethical responsibility, not a one-time certification.
We like to imagine that the therapy room is a sanctuary where we can set aside our assumptions and offer a genuinely clean slate to every client. But the human brain does not work that way. It is a pattern-recognition engine, constantly sorting experience into categories: safe or unsafe, familiar or foreign, like me or not like me.
This cognitive efficiency may have served important evolutionary functions, but in a modern clinical setting it creates a significant blind spot: implicit bias.
Implicit bias refers to automatic, unconscious assumptions that influence our perceptions and decisions without our awareness. These are not the loud, easily identifiable prejudices we can readily examine and challenge. They operate in quiet, split-second moments. The instant assumption that a client who arrives late is “resistant” rather than struggling with an unreliable transport route. The subtle shift in posture when a client describes a lifestyle that feels unfamiliar. The unconscious ranking of whose distress looks urgent and whose appears exaggerated.
The Problem With “Clinical Intuition”
We often confuse bias with clinical intuition. We trust our gut. But research consistently demonstrates that healthcare and mental health providers hold implicit biases at levels comparable to the general population. The crucial difference is that in clinical practice, these biases carry the potential for life-altering consequences.
Consider two clients presenting with identical symptoms. One is a middle-aged professional; the other is a young adult with a history of instability. Without awareness of the process, a clinician’s brain might filter the first client’s irritability as a symptom of depression, triggering empathy, and interpret the second client’s irritability as a sign of substance withdrawal, triggering caution. The diagnosis shifts not because of the clinical data, but because of the narrative the clinician’s brain constructed before the client finished their first sentence. This is not malice; it is cognitive efficiency operating in the wrong context. The result is disparate care.
The American Psychological Association provides evidence-based resources on bias, discrimination, and their clinical impacts that are well worth reviewing.
Interrupting the Pattern
The goal is not to feel guilty about the brain’s categorisation processes, but to interrupt them. Complete elimination of implicit bias is not possible since these processes are neurologically wired. What is possible is actively managing bias through a process called individuation: the conscious work of attending to specific details that contradict the assumed category.
1. The Pause Protocol
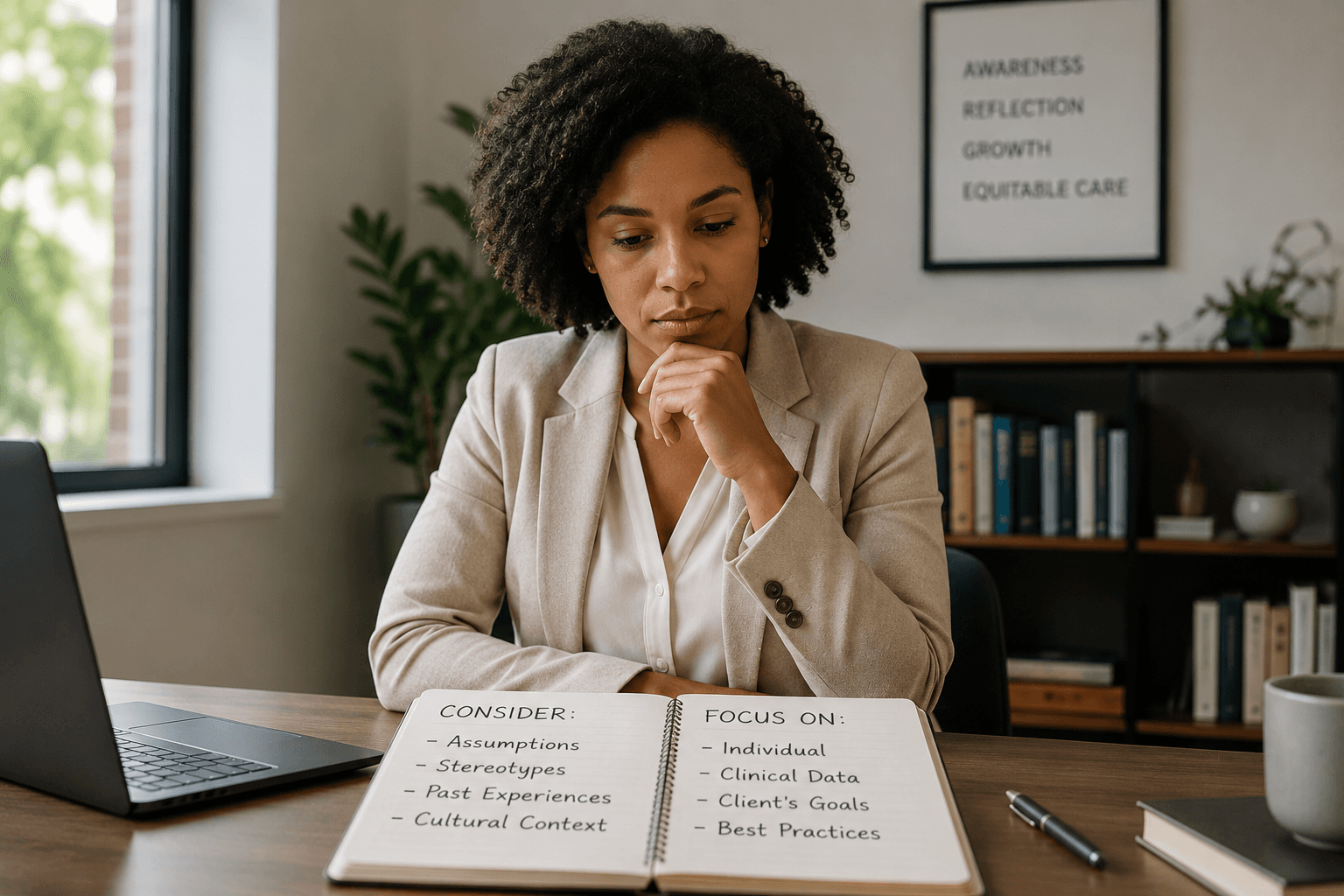
If you notice a strong immediate reaction to a client, whether frustration, fear, or excessive sympathy, treat it as a signal that a bias may have been triggered. Ask yourself: “If this client reminded me of someone I care about, would I be as frustrated? Would I find their story more credible if they spoke differently?” A brief moment of honest self-inquiry is often the only thing standing between a reactive and a genuinely therapeutic response.
2. Diversify Your Reference Points
Cultural competence cannot be developed from textbooks alone. If your practice serves communities that you are not part of, your knowledge should be drawn from those communities’ own voices, not only from clinical studies about them. Actively building a broader cognitive library helps counter the stereotypes that automatic processing relies on.
3. Build Structural Accountability
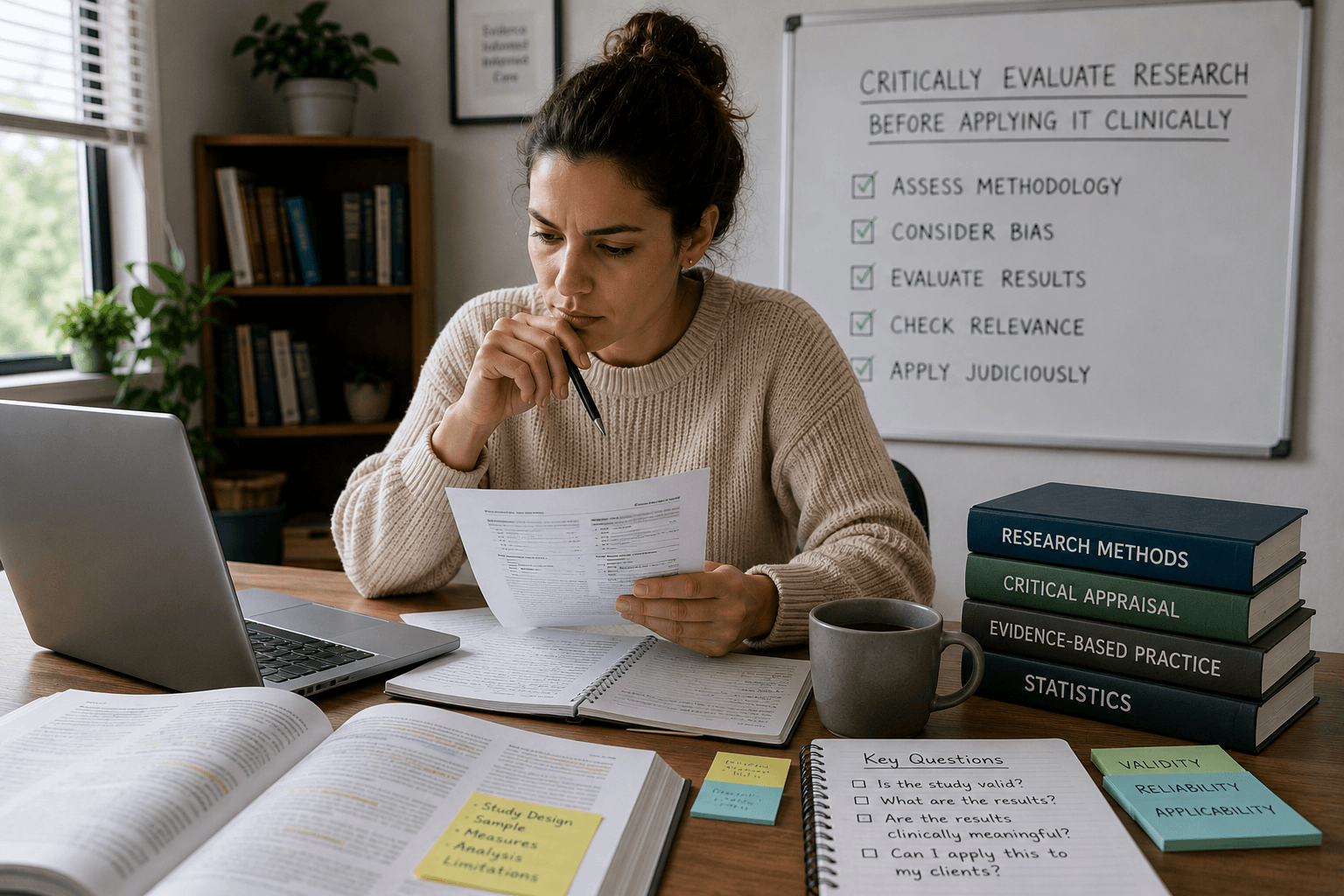
Do not rely solely on willpower. Bias thrives when we are tired, overloaded, or rushed. Build structural safeguards into your practice: use standardized assessment tools rather than gut feeling for diagnostic decisions, and seek supervision when you feel uncertain about a case formulation.
Ethics as Ongoing Practice
Addressing implicit bias is not a one-time certification. It requires a sustained willingness to be wrong and the professional courage to examine aspects of your own thinking that you might not always be comfortable with. This kind of ongoing self-examination moves clinical practice closer to the ethical ideal: seeing the individual in front of you rather than the category you might expect them to represent.
Zur Institute offers a range of courses on cultural competency, ethics, and working with diverse populations. Explore our ethics continuing education for mental health providers to strengthen your clinical judgment.
Frequently Asked Questions
What is implicit bias in mental health practice?
Implicit bias in mental health practice refers to unconscious attitudes and stereotypes that influence a clinician’s perceptions, judgments, and treatment decisions without their deliberate awareness. These biases can affect diagnosis, therapeutic rapport, and the quality of care provided to clients from different backgrounds.
Can implicit bias be eliminated through training?
Research suggests that implicit bias cannot be fully eliminated, but it can be meaningfully reduced and managed through awareness, structured practice, and ongoing self-reflection. Training is most effective when it combines awareness-building with practical skills and structural accountability measures rather than one-off workshops alone.
How does implicit bias affect clinical diagnosis?
Implicit bias can lead clinicians to interpret identical symptoms differently depending on the client’s demographic background, cultural presentation, or personal history. This can result in under-diagnosis, over-diagnosis, or misdiagnosis, particularly in relation to conditions such as depression, anxiety, ADHD, and psychosis, where presentation varies significantly across cultural groups.