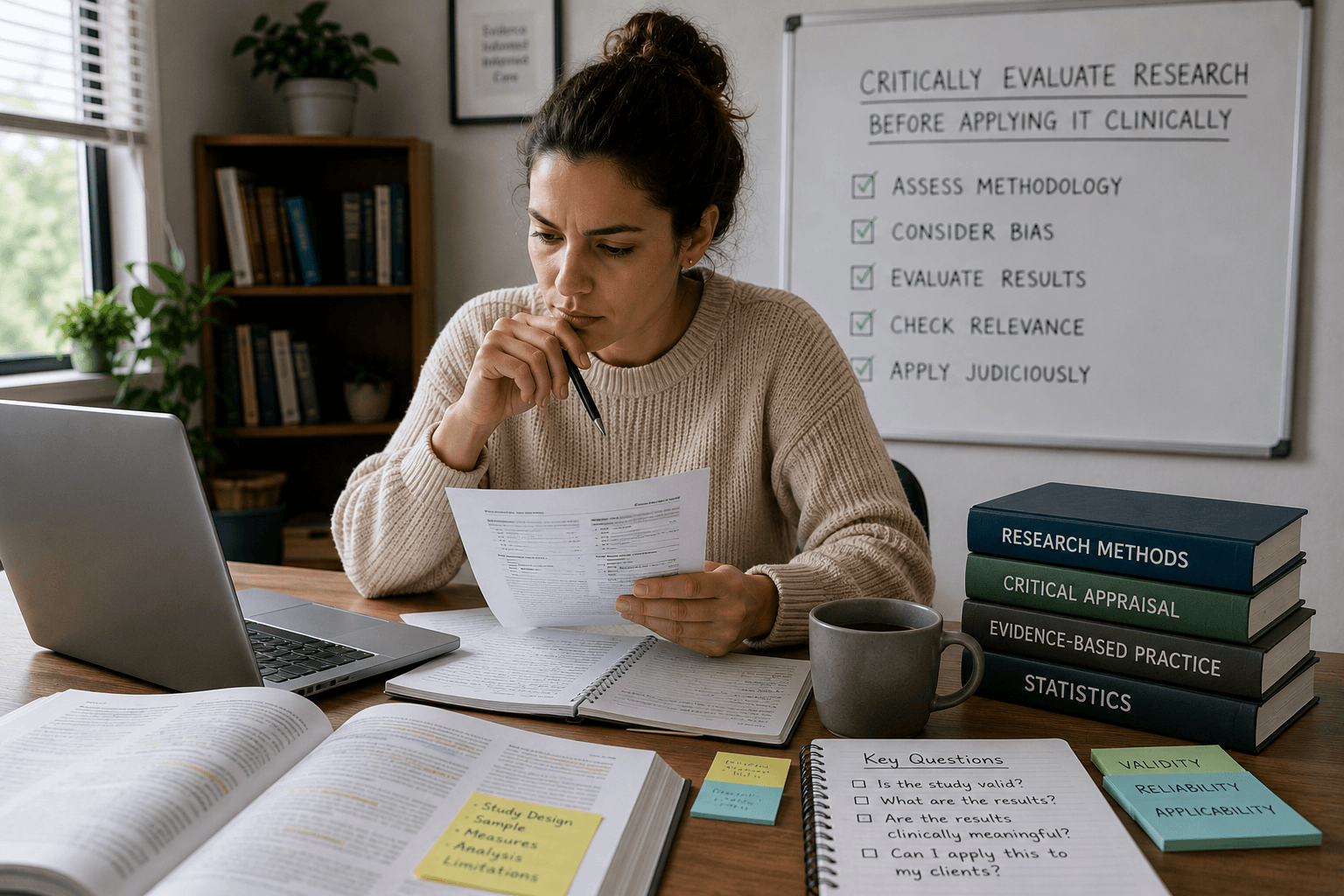
Ethics Continuing EducationHow to Critically Evaluate Research Before Applying It Clinically
We live in an era of “groundbreaking studies.” It seems that every week, a new headline promises a revolution in treating trauma, anxiety, or addiction. For clinicians, this constant stream of new findings is both promising and exhausting. We want to offer our clients the best care possible, but we also know that not all […] Read More…
May 24