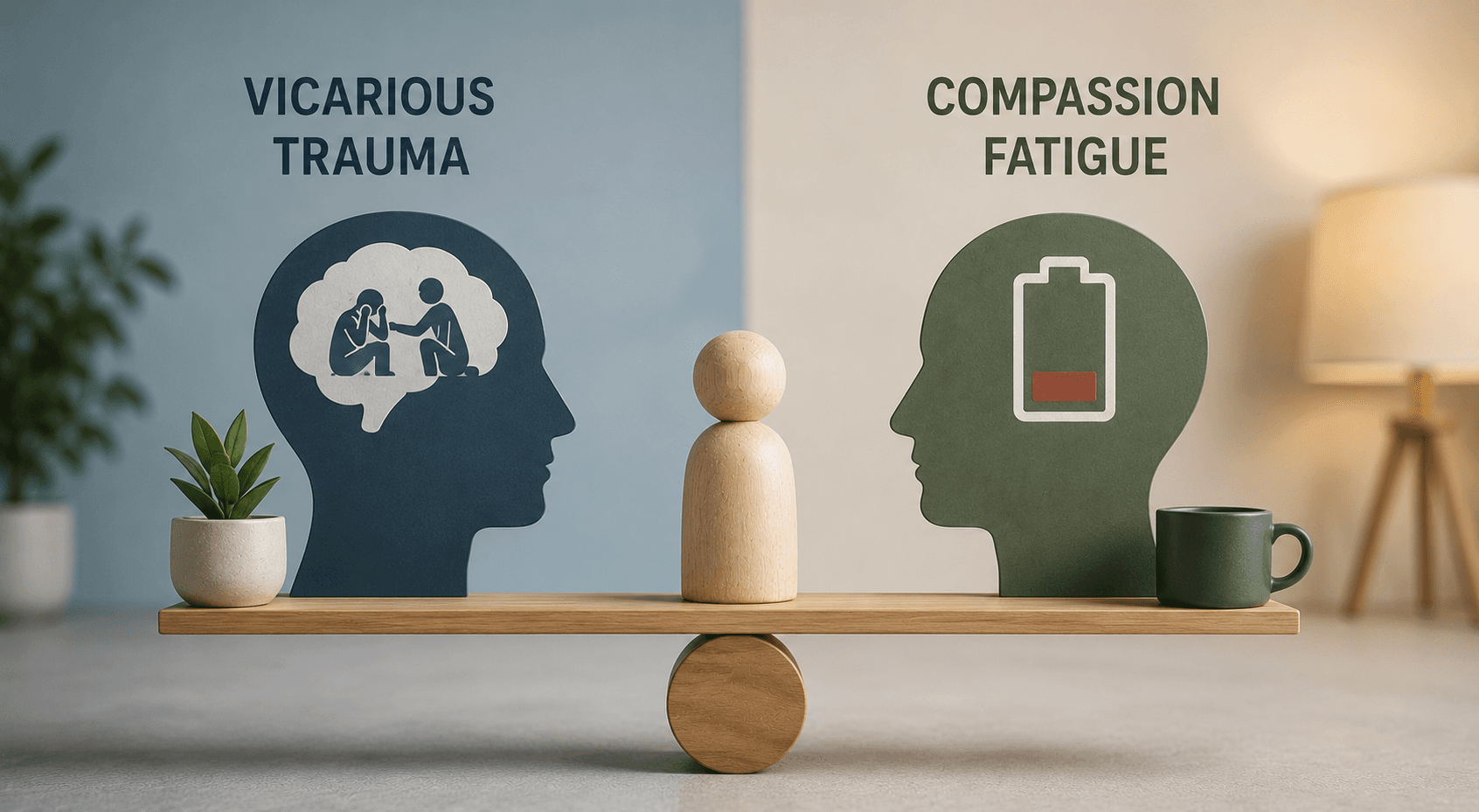
- Compassion fatigue is the gradual erosion of emotional bandwidth; it often feels like muffled empathy or emotional flatness after repeated exposure to clients in distress.
- Vicarious trauma is deeper and involves a noticeable shift in the clinician’s worldview, sense of safety, or perception of others.
- The two conditions require different responses: compassion fatigue often improves with lifestyle adjustments, while vicarious trauma typically requires more active support.
- Regular supervision, peer consultation, and self-monitoring are protective factors for both conditions.
- Recognising the difference early is key to preventing long-term professional and personal harm.
There is a moment in clinical work, usually after you have been doing it long enough that others assume you are “used to it,” when you realise the work has started to live in your body. Maybe you sit in your car after a session, hands on the steering wheel, simply staring into the distance. Or you finally get home and feel like your nervous system has completely shut down. Most clinicians have had some version of this experience.
Two conditions tend to be responsible: compassion fatigue and vicarious trauma. They sound similar and can feel similar when you are in the middle of them. But they are not the same, and understanding the difference can make your work, and your life outside it, more manageable.
What Compassion Fatigue Feels Like
Compassion fatigue is the slow, quiet erosion of your emotional capacity for empathy. It does not arrive all at once. It is more like sitting with a client you care deeply about, someone you normally feel fully connected to, and noticing you have to work to access that connection. Your empathy is still there, just muffled, as though it is behind a door that quietly closed without you noticing.
This is distinct from administrative burnout. You can be completely on top of your workload and still experience this kind of emotional flatness.
Common signs clinicians report include:
- Feeling emotionally depleted after sessions that previously felt manageable.
- Irritability arising where patience used to come naturally.
- A sense of numbness or of being technically present but not fully engaged.
- Persistent thoughts like “Am I actually helping anyone?”
How Vicarious Trauma Shows Up
Vicarious trauma runs deeper and affects differently. It is not simply feeling tired or stretched thin. It is the way certain client stories begin to shift how you perceive the world, not in the “I need a holiday” sense, but in the “I no longer trust my environment the way I once did” sense.
You might find yourself checking your locks more carefully at night, or noticing that certain topics in the news hit harder than they once did. You may catch yourself thinking about a client’s trauma during ordinary daily activities such as washing dishes or doing the grocery shopping.
Common signs include:
- Heightened alertness, suspicion, or a persistent sense of unease.
- Intrusive thoughts or mental images connected to clients’ trauma narratives.
- A noticeable shift in your broader worldview or sense of personal safety.
- Difficulty maintaining a clear boundary between your own life and the trauma you hear about in sessions.
Vicarious trauma does not resolve with a long weekend. It typically requires honest conversation, structured reflection, and sometimes personal therapy to process what has accumulated. The American Psychological Association recognises it as a significant occupational hazard for mental health professionals.
Key Differences at a Glance
| Feature | Compassion Fatigue | Vicarious Trauma |
|---|---|---|
| Primary experience | Emotional exhaustion and reduced empathy | Shift in worldview and sense of safety |
| Onset | Gradual erosion over time | Can develop after repeated exposure to traumatic content |
| Intrusive symptoms | Less common | Intrusive thoughts and images are typical |
| Resolution | Often responds to lifestyle and schedule adjustments | Typically requires supervision, therapy, or structured support |
Why Making the Distinction Matters
Knowing what you are dealing with is not about attaching a label to yourself. It is about understanding why you have been feeling off and recognising that you are not losing your clinical edge; you are carrying significant emotional weight.
Compassion fatigue often softens when day-to-day rhythms are adjusted: spacing out sessions to allow breathing room, setting firmer limits on out-of-hours contact, or simply doing things that reconnect you to your life outside the therapy room.
Vicarious trauma needs more intentional attention. Talking things through with a trusted person, exploring therapy continuing education courses for new clinical tools, or working with your own therapist can all help. It is not a sign that you are in the wrong profession. It is the professional equivalent of recognising you need maintenance before something breaks down entirely.
Taking Care of Yourself as You Care for Clients
These experiences are common at every stage of a clinical career, regardless of how seasoned or grounded you are. The goal is not to be unaffected by the work. It is to notice the impact early and respond before it becomes entrenched.
Protective strategies include:
- Talking regularly with a trusted colleague, peer group, or a supervisor with solid clinical supervision training.
- Grounding or mindfulness practices between client sessions.
- Honest, regular self-monitoring about how the work is affecting you.
- Clear limits that protect your personal time and energy.
These are not signs of weakness. They are indicators of ethical, sustainable clinical practice, and ongoing ethics continuing education reinforces this responsibility.
If this topic resonates with you, Zur Institute offers trainings that explore these themes in depth and provide practical tools for everyday practice. If you would like guidance on where to start, get in touch and we will help you find the right fit.
Frequently Asked Questions
What is the main difference between vicarious trauma and compassion fatigue?
Compassion fatigue primarily affects a clinician’s emotional energy and empathic capacity. Vicarious trauma is more pervasive and involves lasting changes to a clinician’s worldview, sense of safety, and beliefs about the world, resulting from repeated exposure to clients’ traumatic material.
Can vicarious trauma and compassion fatigue occur at the same time?
Yes. Clinicians can experience elements of both simultaneously. In fact, compassion fatigue can sometimes be a precursor to vicarious trauma if left unaddressed, as chronic emotional depletion reduces resilience and increases vulnerability to deeper impact.
How do I know if I need professional support for vicarious trauma?
If you are experiencing intrusive thoughts related to clients’ stories, a persistent shift in how you perceive the world or others, difficulty sleeping, or a sense that your personal relationships are being affected by what you hear in sessions, these are signs that peer consultation or personal therapy would be beneficial.